Swallowing is something most of us do without thinking. For people with achalasia cardia, that simple habit can become a daily struggle. Over the past decade, a minimally invasive endoscopic treatment called POEM (per-oral endoscopic myotomy) has transformed how we treat achalasia. This post breaks down what achalasia is, how it’s diagnosed, what POEM involves, its benefits and risks, and what patients can expect — presented in clear, patient-friendly language.
By : Dr. Surakshith T K
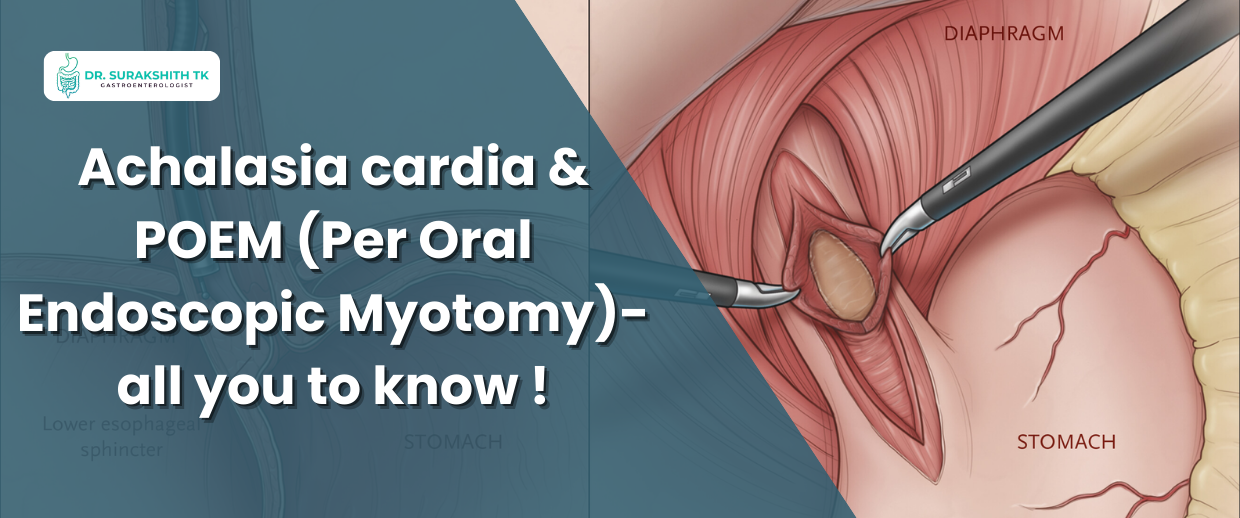
What is achalasia cardia?
Achalasia is a disorder of the esophagus in which the lower esophageal sphincter (LES) — the valve between the food pipe and the stomach — fails to relax properly, and the esophagus loses normal coordinated contractions. The result: food and liquids don’t pass smoothly into the stomach and may accumulate, causing symptoms that usually worsen gradually over time. Common symptoms include difficulty swallowing (solids and liquids), regurgitation, chest pain, heartburn-like symptoms, coughing, and weight loss.
How is achalasia diagnosed?
Diagnosis typically uses a combination of tests:
High-resolution esophageal manometry (HRM) — the gold standard; it measures esophageal muscle contractions and LES relaxation.
Barium swallow (timed barium esophagram) — shows how the esophagus fills and empties and helps assess the severity and shape (including advanced or sigmoid esophagus).
Upper endoscopy (EGD) — rules out mechanical blockage (like a tumor) and checks for retained food or inflammation.
These tests together help classify achalasia into subtypes, which guide treatment choice.
Treatment options — where does POEM fit?
Treatment aims to relieve the functional obstruction at the LES. Options include:
Botulinum toxin injection into the LES (short-lasting relief, often for patients unfit for surgery).
Pneumatic dilation (balloon dilatation of the LES).
Laparoscopic Heller myotomy (LHM) with partial fundoplication (surgery to cut the muscle and add an anti-reflux wrap).
POEM (Per-Oral Endoscopic Myotomy) — an endoscopic, tunnel-based myotomy performed through the mouth.
POEM has rapidly become a mainstay for many patients because it is minimally invasive, highly effective in relieving dysphagia, and can be tailored in length depending on disease pattern.
What exactly is POEM? (A step-by-step look)
POEM is performed under general anesthesia by an experienced endoscopist:
The endoscope is passed into the esophagus.
A small incision is made in the mucosa (inner lining).
A submucosal tunnel is created between the mucosal and muscular layers down to and slightly into the stomach.
The circular muscle fibers of the LES and lower esophagus are selectively cut (myotomy), relieving the outflow obstruction.
The mucosal entry is closed with clips.
Because POEM uses a “third-space” endoscopic approach, it avoids external incisions and usually leads to shorter hospital stay and quicker recovery.
Who is a good candidate?
POEM is suitable for adults with achalasia of all subtypes, including patients who previously failed pneumatic dilation or Heller myotomy. It’s also used increasingly for certain spastic motility disorders and advanced achalasia (including sigmoid esophagus) by experienced teams. Individual evaluation with HRM, imaging, and endoscopy is essential to choose the best option.
Benefits — why choose POEM?
Excellent symptom relief and reduction in Eckardt scores (a clinical symptom score).
Flexible myotomy length — can be extended to treat long segment disease or spastic segments.
Minimally invasive — no external scar; often shorter hospital stays and faster return to normal activities compared with open surgery.
Comparative studies and guidelines now support POEM as an effective alternative to surgical myotomy in appropriately selected patients.
Risks & considerations (what you must know)
Gastroesophageal reflux disease (GERD) after POEM is more common than after Heller myotomy with fundoplication because POEM does not include an anti-reflux surgical wrap; many patients require acid suppression (PPI) after POEM. Long-term reflux monitoring may be needed.
Procedure-related risks include bleeding, mucosal injury, and, rarely, infection or perforation — but serious complications are uncommon when performed by experienced teams.
Long-term (decade-long) outcome data are still maturing, although current evidence shows durable symptom relief for the majority of patients.
Recovery & follow-up — what to expect
Most patients stay in hospital a short time (often 1–2 days). A liquid diet is started and gradually advanced. Proton pump inhibitors (PPIs) are commonly prescribed to manage reflux. Follow-up usually includes symptom checks, manometry or timed barium studies in selected cases, and endoscopy if reflux or other complications are suspected.
Final thoughts from Dr. Surakshit T K
Achalasia can be life-altering, but modern diagnostics and treatments — especially POEM — offer excellent chances of restoring comfortable swallowing and quality of life. POEM is not a one-size-fits-all cure; candidacy and approach should be individualized after careful testing and discussion of risks (notably reflux). If you or a loved one are experiencing progressive difficulty swallowing, persistent regurgitation, or unexplained weight loss, early evaluation by a gastroenterologist with expertise in motility disorders is the right first step.
If you'd like a tailored consultation or a second opinion about achalasia and whether POEM is appropriate for you, my clinic evaluates patients using HRM, imaging, and endoscopy to design a safe, evidence-based plan. — Dr. Surakshit T K
Dr. Surakshith T K
Specialist Gastroenterologist and Hepatologist
Dr. Surakshith T K is a leading gastroenterologist and hepatologist
with 12+ years of experience, specializing in advanced endoscopic procedures including
POEM, ERCP, EUS, ESD/EMR, and bariatric endoscopy. He is known for expert care in GI,
liver, pancreatic, and biliary disorders with a strong focus on early cancer detection.